PSA, Gleason score, active surveillance, radical prostatectomy, radiation, and hormone therapy
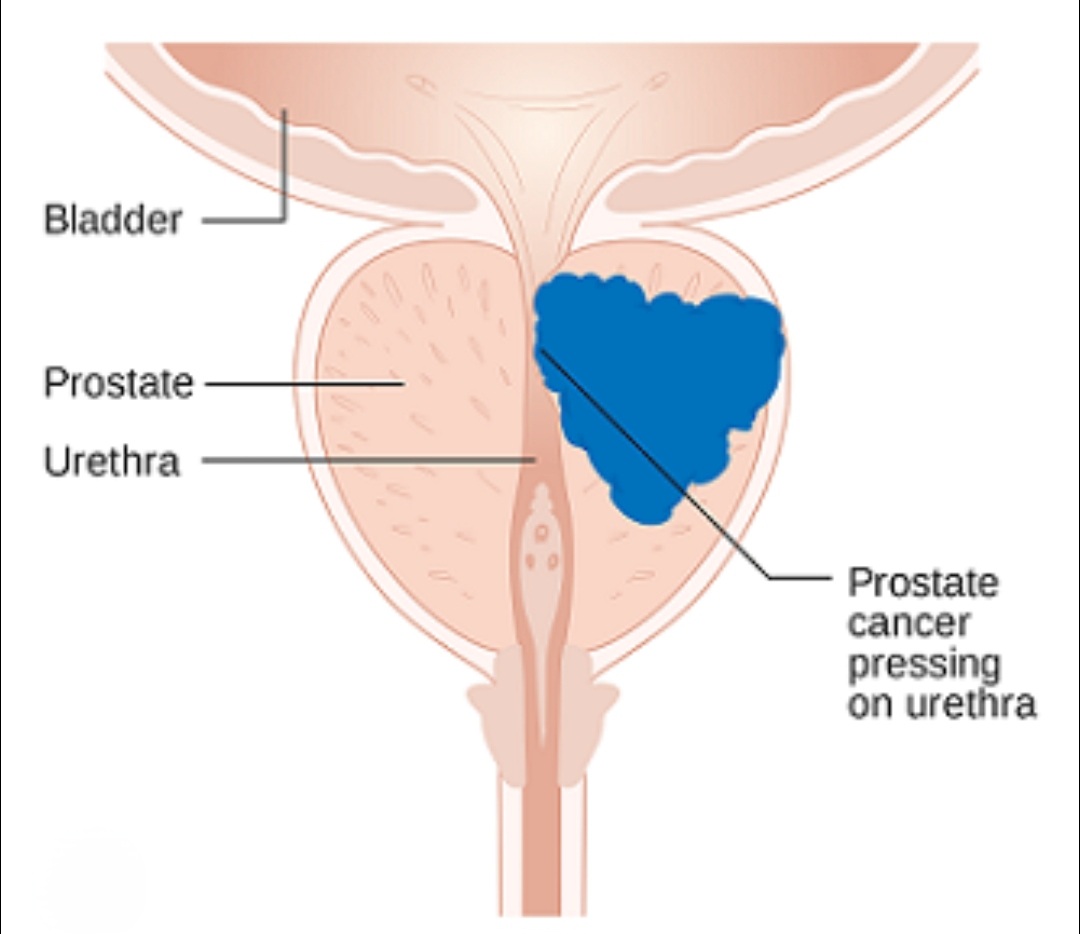
Prostate cancer is malignant growth in the prostate gland, usually adenocarcinoma. It is the most common cancer in men. Most cases are slow-growing and detected before causing symptoms. The challenge is distinguishing clinically significant cancers needing treatment from indolent ones managed conservatively.
PSA (Prostate-Specific Antigen) is a protein produced by prostate cells. Elevated PSA (>4 ng/mL) or rapidly rising PSA prompts further evaluation. PSA density (PSA/prostate volume), PSA velocity, and free-to-total PSA ratio improve specificity. PSA screening in men 50-70 (or 45 with family history) is recommended after shared decision-making.
The Gleason score grades how abnormal prostate cancer cells look under a microscope (1-5 scale). The two most common patterns are added to give a score out of 10. Gleason 6 (3+3): low grade, slow-growing. Gleason 7 (3+4 or 4+3): intermediate. Gleason 8-10: high grade, aggressive. The Grade Group system (1-5) is now preferred.
MRI prostate (mpMRI) identifies suspicious lesions and guides targeted biopsy. Transrectal or transperineal biopsy (12-16 cores, TRUS-guided or cognitive/fusion) confirms diagnosis. Staging uses CT and bone scan or PSMA-PET for high-risk cases. Clinical staging: T1-T2 (localized), T3-T4 (locally advanced), M1 (metastatic).
Active surveillance monitors low-risk prostate cancer with regular PSA, MRI, and repeat biopsies (at 1 year, then every 2-3 years) without immediate treatment. It avoids overtreatment and preserves quality of life. About 50% of low-risk patients remain on surveillance long-term; the rest are converted to treatment when the cancer shows signs of progression.
Have more questions? Book a consultation with Dr. Samer Morsy
Radical prostatectomy removes the entire prostate and seminal vesicles. Robotic-assisted (RARP) and open approaches are available. Nerve-sparing techniques preserve erectile function in 50-80%. Urinary incontinence affects 5-20% long-term. 5-year biochemical recurrence-free survival for localized disease exceeds 85%.
External beam radiotherapy (EBRT/IMRT) delivers precise radiation over 4-8 weeks. Stereotactic body radiotherapy (SBRT) treats in 5 sessions. Brachytherapy implants radioactive seeds permanently or temporarily. Radiation is equivalent to surgery for localized cancer but side effects differ. ADT is added for high-risk disease.
Androgen deprivation therapy (ADT) lowers testosterone to starve cancer cells. Medical castration uses LHRH agonists (leuprolide) or antagonists (degarelix). Anti-androgens (bicalutamide, enzalutamide) block testosterone receptors. ADT is used for metastatic, high-risk localized, and biochemically recurrent disease. Side effects: hot flashes, bone loss, metabolic syndrome.
BPH (benign prostatic hyperplasia) and prostate cancer can coexist. BPH causes obstructive symptoms (weak stream, frequency) but is not cancer. Key differences: BPH does not spread; prostate cancer can be asymptomatic early. PSA is elevated in both. An enlarged prostate on DRE does not distinguish them — biopsy is needed for definitive diagnosis.
Localized prostate cancer: 5-year survival nearly 100%. Regional disease: 5-year survival >95%. Distant metastasis: 5-year survival 30%. With modern treatments including novel hormonal agents (enzalutamide, abiraterone), PSMA-targeted radioligand therapy, and immunotherapy, even metastatic disease has improving outcomes. Early detection remains the key.
Ready to take the next step? Book your appointment today