Causes, semen analysis, varicocele, surgical sperm retrieval, and IVF/ICSI outcomes
Male infertility is the inability to achieve pregnancy in a fertile female partner after 12 months of regular unprotected intercourse. It contributes to about 50% of infertility cases. Male factors include low sperm count, poor motility, abnormal morphology, or complete absence of sperm (azoospermia).
Normal values (WHO 2021): sperm count >16 million/mL, total motility >42%, progressive motility >30%, morphology (Kruger strict) >4% normal forms. A single abnormal result should be confirmed with a repeat test 2-3 months later. Three analyses may be needed for accuracy.
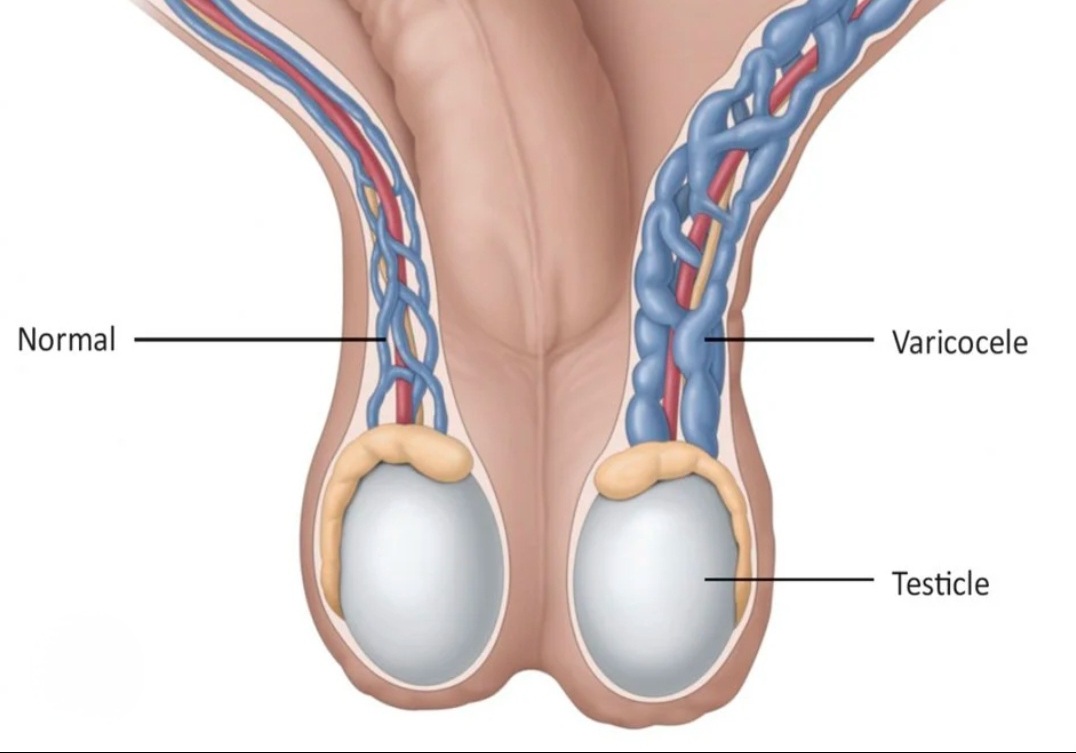
Varicocele (dilated testicular veins, most common treatable cause), hormonal imbalances (low FSH/LH/testosterone), genetic causes (Klinefelter syndrome, Y-chromosome microdeletions), obstruction, previous infections, undescended testis, radiation/chemotherapy, and lifestyle factors.
FSH, LH, testosterone, prolactin, and estradiol form the basic hormonal panel. Elevated FSH with azoospermia suggests testicular failure. Low FSH suggests hypothalamic-pituitary problem treatable with gonadotropins. Testosterone below 12 nmol/L requires treatment.
Varicocele (dilated veins around the testicle) is found in 40% of infertile men. It raises testicular temperature, reducing sperm production. Surgical ligation or microsurgical varicocelectomy improves semen parameters in 60-80% of cases and achieves spontaneous pregnancy in 30-40% within 2 years.
Have more questions? Book a consultation with Dr. Samer Morsy
For azoospermia: PESA (percutaneous epididymal sperm aspiration) for obstructive cases, TESA (testicular aspiration) for simple cases, conventional TESE (testicular biopsy), and Micro-TESE (microsurgical extraction) for non-obstructive azoospermia with the highest success rate (40-60%).
IVF (in vitro fertilization) fertilizes eggs outside the body. ICSI (intracytoplasmic sperm injection) injects a single sperm directly into an egg — it is used for severe male factor infertility and achieves similar fertilization rates even with very few sperm. Success rates depend on female age.
Heat damages sperm (avoid hot baths, laptops on lap, tight underwear). Smoking reduces count and motility. Obesity lowers testosterone. Anabolic steroids cause testicular atrophy. Antioxidants (vitamin C, E, zinc, selenium, CoQ10) may improve semen parameters.
Varicocele repair: 30-40% spontaneous pregnancy in 2 years. IVF/ICSI per cycle: 30-50% (varies by female age and embryo quality). Micro-TESE sperm retrieval: 40-60%. Early diagnosis and treatment by a specialized andrologist significantly improves outcomes.
After 12 months of trying (or 6 months if the female partner is over 35). Immediately if there is a known risk factor: previous mumps orchitis, undescended testis, prior chemotherapy, or varicocele. A simple semen analysis is the first step and can be arranged quickly.
Ready to take the next step? Book your appointment today