Symptoms, staging, TURBT, intravesical therapy, and radical cystectomy explained
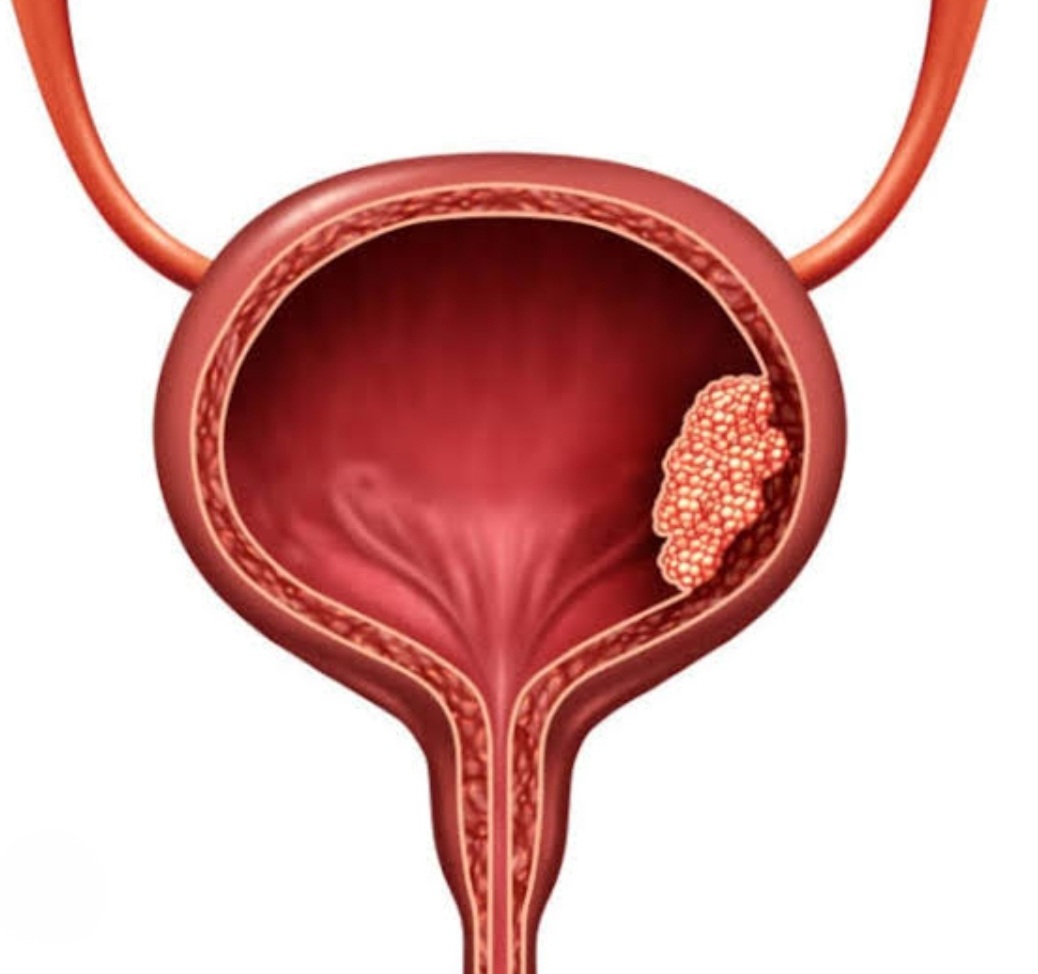
Bladder cancer is the uncontrolled growth of cells in the bladder lining (urothelium). It is the most common urinary tract cancer. About 75% are non-muscle-invasive at diagnosis (NMIBC — stages Ta, T1, CIS) and 25% are muscle-invasive (MIBC — T2 and above). Men are 3-4 times more likely to develop it than women.
Painless blood in urine (hematuria) is the most common sign, occurring in 80-90% of cases. Other signs: frequent urination, burning during urination, and urgency. Blood in urine should always be investigated urgently — it should not be assumed to be from a benign cause without cystoscopy.
Smoking is the single largest risk factor (50% of cases) — smokers have a 3x higher risk. Occupational exposure to aromatic amines (painters, hairdressers, rubber workers). Chronic bladder infections (especially with Schistosoma haematobium in endemic areas like Egypt). Previous pelvic radiation and cyclophosphamide chemotherapy also increase risk.
Cystoscopy (direct visualization of the bladder) is the gold standard. Urine cytology detects shed cancer cells. CT urogram maps the upper urinary tract. Urine biomarkers (NMP22, UroVysion FISH) supplement diagnosis. Biopsy confirms the diagnosis and stage. Bimanual examination under anesthesia assesses extent.
Transurethral Resection of Bladder Tumor (TURBT) is the primary treatment for non-muscle-invasive bladder cancer. A resectoscope passes through the urethra to remove visible tumors. It is performed under spinal or general anesthesia. A second TURBT 4-6 weeks later is recommended for T1 and high-grade tumors to ensure complete resection.
Have more questions? Book a consultation with Dr. Samer Morsy
BCG (Bacillus Calmette-Guerin) is an immunotherapy instilled directly into the bladder after TURBT for intermediate and high-risk NMIBC. It reduces recurrence by 30-40% and progression risk. A 6-week induction course followed by 1-3 year maintenance is standard. Side effects include bladder irritation, flu-like symptoms, and rarely systemic BCG infection.
Radical cystectomy (bladder removal) is the standard treatment for muscle-invasive bladder cancer. In men, the prostate and seminal vesicles are removed; in women, the uterus and ovaries. Urinary diversion is then performed: ileal conduit (urostomy bag), orthotopic neobladder (using bowel, allows normal urination), or continent pouch.
Cisplatin-based chemotherapy given before cystectomy shrinks the tumor, kills micrometastases, and improves 5-year survival by 5-8%. It is recommended for all fit patients with muscle-invasive disease. MVAC (methotrexate, vinblastine, adriamycin, cisplatin) or gemcitabine-cisplatin are standard regimens.
5-year survival: stage Ta/T1 (NMIBC) over 90% with proper treatment. Stage T2: 50-65% after radical cystectomy. Stage T3: 30-50%. Stage T4 (metastatic): 5-15%. Regular follow-up cystoscopy (every 3 months for 2 years) is critical as NMIBC has a 50-70% recurrence rate.
Non-muscle-invasive: cystoscopy every 3 months for 2 years, then every 6 months for 2 years, then annually. Upper tract imaging yearly. After cystectomy: CT chest/abdomen/pelvis every 6 months for 2-3 years, then annually. Urine cytology at each visit. Lifelong surveillance is essential.
Ready to take the next step? Book your appointment today